20 Borderline Personality Disorder Statistics for 2025
Borderline personality disorder (BPD) is one of the most challenging and often misunderstood mental health conditions. It’s characterized by intense emotional instability, difficulty maintaining relationships, and a fragile sense of self.
Individuals with BPD experience pervasive patterns of mood swings, impulsivity, and fear of abandonment that can cause significant distress, damage interpersonal relationships, and impair daily functioning.
To receive a diagnosis of BPD, a person must meet at least five diagnostic criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). These include:
- Desperate efforts to avoid abandonment, whether real or imagined
- Intense, unstable relationships that shift between idealizing and devaluing others.
- Unstable or distorted sense of self
- At least two impulsive behaviors that may cause self-harm, such as substance use, binge eating, reckless driving, risky sex, or irresponsible spending
- Repeated suicidal behavior, threats, or self-harm
- Rapidly shifting moods, such as intense sadness, irritability, or anxiety
- Ongoing feelings of emptiness
- Poorly controlled or intense anger
- Brief, stress-related paranoia or dissociation
Because of its complexity, BPD is an important focus in many continuing education courses, which help clinicians and providers stay updated on evolving best practices in diagnosis, treatment, and care. We’ve compiled 20 borderline personality disorder statistics that provide insights into its prevalence, prognosis, and the serious risks it presents—including suicidal and self-harming behavior.
Key Borderline Personality Disorder Statistics
1. At least 1.6% of Americans have borderline personality disorder (source)

Studies indicate that 1.6% of the adult U.S. population, or 4 million people, have borderline personality disorder. However, researchers believe this may be an underestimate, and the true percentage may be as high as 5.9%.
2. Women are more likely to be diagnosed with BPD, representing nearly 75% of diagnoses in the U.S. (source)
Approximately three-fourths of Americans diagnosed with borderline personality disorder are female. However, gender differences in diagnosis may obscure the true prevalence of the disorder among men, who are often misdiagnosed with other conditions such as depression or post-traumatic stress disorder (PTSD). Gender differences in how behaviors like anger, aggression, promiscuity, and disordered eating are perceived can also contribute to these diagnostic disparities.
3. People in inpatient psychiatric settings are much more likely to have BPD than people in outpatient clinics (source)
Borderline personality disorder is diagnosed in about 20–22% of people in psychiatric inpatient settings, compared to 10–12% of people in outpatient psychiatric clinics. More research is needed to understand how common BPD is in other healthcare environments, like primary care, and how factors like age, gender, or background may affect its prevalence.
Borderline Personality Disorder Statistics – Suicide and Mortality Risk
4. Around 75% of people with BPD attempt suicide at least once in their lives (source)
Borderline personality disorder statistics show similar rates of people who have attempted suicide among both adults and adolescents. However, adults are more likely to attempt suicide five or more times.
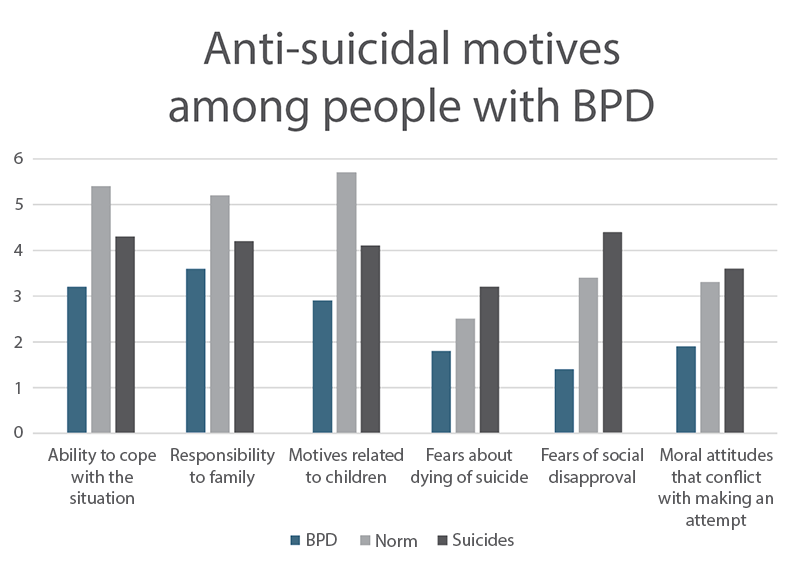
Among those who resist suicidal urges, the most common reason is a sense of responsibility to family—a powerful protective factor clinicians should be aware of when assessing risk.
5. 5.9% of people with borderline personality disorder die by suicide (source)
Nearly 6% of people with BPD will complete suicide—a rate higher than individuals with other personality disorders (1.4% on average). Over periods of 5 to 14 years, 2% to 5% of people with BPD committed suicide, with a mean of 4%.
6. People with BPD who die by suicide tend to do so after years of ineffective treatment—around age 30 to 37 (source)
A 15-year follow-back study found the mean age at suicide to be 30, while a 27-year follow-up study reported a mean age of 37, with a standard deviation of 10. This challenges the assumption that suicide risk in BPD peaks during early adulthood, when patients are more frequently seen in emergency settings.
Despite this long window of clinical contact, no research has shown that suicide prevention efforts in BPD are effective, and hospitalization has not been found to reduce risk.
Borderline Personality Disorder Statistics – Causes and Risk Factors
7. Genetics may play a role in BPD, with about 40% of the risk believed to be inherited (source)
Family and twin studies suggest a genetic influence, but specific genes haven’t been clearly linked to the disorder. Some researchers think genes may increase sensitivity to both positive and negative life experiences, rather than directly causing BPD. Borderline personality disorder likely develops through a mix of genetic vulnerability and adverse childhood experiences, such as neglect or abuse.
8. Between 30% and 90% of people with BPD have a history of childhood abuse or neglect (source)
This percentage is significantly higher than in other personality disorders. These early experiences often disrupt emotional development, making it harder to manage feelings and form healthy relationships later in life.
When children grow up without emotional support or consistent care, they may develop a negative view of themselves and others. They often expect rejection or mistreatment in future relationships. Over time, this can lead to intense emotional swings and difficulty expressing or controlling emotions—hallmarks of BPD.
9. About 44% of people with BPD experienced childhood sexual abuse (source)
This aligns with earlier research showing rates between 40% and 70%. Differences in findings may be due to how patients were selected, how BPD and abuse were diagnosed, or cultural factors. While childhood sexual abuse (CSA) isn’t the only cause of BPD—and not all people with BPD have this history—it appears to be a significant risk factor in many cases.
Borderline Personality Disorder Statistics – Adolescents
10. Around 3% of adolescents in the general population have borderline personality disorder (source)
Rates are much higher in clinical settings—about 11% in outpatient clinics and up to 78% among suicidal teens in emergency care. Diagnosis is based on clinical evaluation, considering emotional development and relationships, with symptoms lasting at least one year. BPD has been identified in adolescents as young as 11 years old.
11. Extreme self-harm is more common in adolescents with BPD than in adults (source)
While about 90% of both teens and adults with borderline personality disorder have self-harmed, adolescents are more likely to report very high numbers of self-injury episodes—sometimes over 25 or even 50 times. Cutting is especially more frequent among teens.
12. 68% of adolescents admitted to the ER after a suicide attempt have BPD (source)
Suicidal ideation is present in 59% of teens with BPD, and self-injury in 58%. These behaviors are more common in teens with BPD than in those without. Doctors should always assess for BPD when teens show signs of suicidal behavior, self-harm, frequent unexplained physical symptoms, or poor follow-through with medical care.
13. Childhood ADHD and ODD are strong predictors of borderline personality disorder symptoms in adolescence (source)
Children—particularly those with attention-deficit/hyperactivity disorder (ADHD) or oppositional defiant disorder (ODD)—are at increased risk of developing BPD symptoms during their teenage years:
- In male adolescent outpatients, only childhood ADHD and ODD predicted later BPD symptoms.
- Girls aged 8–10 with ODD, and 10–13 with ADHD, are more likely to show BPD symptoms by age 14.
These results underline the impact of externalizing disorders—especially ODD—on personality development and reinforce the importance of early screening and preventive care for at-risk children.
14. Many adolescents with BPD remit within 4 years—yet 76% of high-risk teens still show symptoms (source)
The majority of adolescents with early-onset BPD improve enough that they no longer fit the diagnosis within four years. However, a study of suicidal adolescent girls with BPD revealed that about three-fourths of them still had some symptoms at the end of that timeframe.
Clinical studies indicate adolescents with early onset, severe BPD are the most at risk of remaining symptomatic into adulthood. Factors associated with BPD persistence include:
- Emotional instability: Unstable relationships, self-image, and mood.
- Family dynamics: BPD in the mother, substance use disorder (SUD) in the father, and high levels of mother–child conflict.
- Adolescent comorbidities: Depression (DDs) and substance use disorders (SUDs)
- Clinical profile: Early onset of BPD, suicidality in adolescence, and co-occurring externalizing and internalizing disorders, although analysis showed only DDs and SUDs predicted BPD in adulthood.
These findings suggest that both psychological and family-related factors play a role in the long-term trajectory of BPD, and that early intervention—especially targeting mood and substance issues—may help improve outcomes.
Borderline Personality Disorder Statistics – Prognosis, Treatment, and Complications
15. The life expectancy for people with BPD is 20 years less than the national average (source)
This gap isn’t just due to mental health challenges—it also reflects serious impacts on physical health, especially cardiovascular issues. Risk factors include substance use, self-harm, suicide, poor sexual health, and exposure to blood-borne illnesses.
Lifestyle factors like smoking, inactivity, poor diet, and obesity also play a role, along with the use of certain medications—such as opioids, benzodiazepines, or some psychiatric drugs—that may further strain the body, particularly the metabolic and cardiovascular systems.
16. Nearly 50% of people with BPD don’t respond fully to psychotherapy (source)
While psychotherapy is the most effective treatment for borderline personality disorder, more than half of patients do not respond sufficiently. Several therapy types—like dialectical behavior therapy and schema therapy—can help reduce symptoms, but no single method works best for everyone.
Medications may help with related issues like anxiety or depression, but they don’t treat the core symptoms of BPD. Early diagnosis and treatment can improve outcomes, but more research is still needed.
17. Up to 96% of people treated for BPD are prescribed at least one psychotropic medication—even though no medications are officially approved (source)
In fact, nearly 19% are prescribed four or more psychotropic medications at once. Health organizations in both the UK and Australia advise against using medication as a first-line treatment except during acute crises. Other professional bodies support limited use of antipsychotics and mood stabilizers to target specific symptoms—such as anger, impulsivity, or mood instability—or to manage co-occurring conditions like anxiety and depression.
Effective BPD treatment options include a combination of psychotherapy, psychiatry, medication, and support from family members and loved ones. Cognitive behavioral therapy (CBT) and specialized approaches like mentalization-based treatment (MBT) are common strategies. Success can depend on the individual’s willingness to engage—a factor often measured in clinical research by degree of improvement (DOI).
18. Depression and anxiety disorders are the most common comorbidities for people with BPD, and rates tend to be slightly higher in women (source)
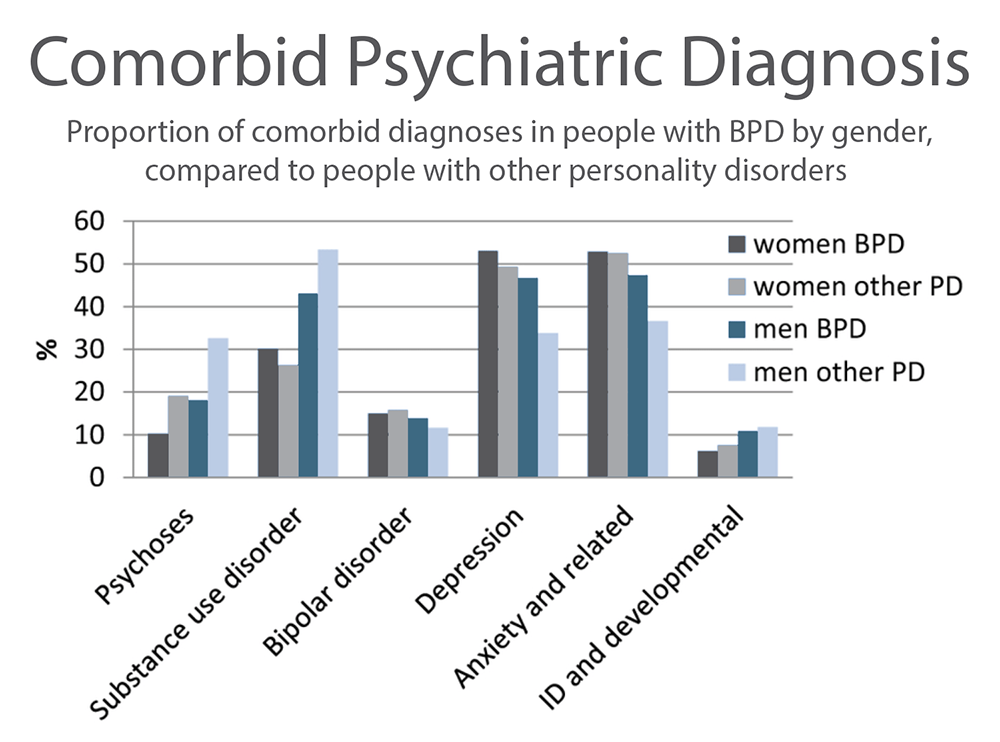
Common comorbidities for people with borderline personality disorder include psychoses, substance use disorder, bipolar disorder, depression, anxiety disorders, and intellectual disability (ID) and developmental disorders.
Rates of depression and anxiety disorders are higher in patients with BPD, particularly in men, compared to people with other personality disorders (PD). However, psychoses are significantly less common in both men and women with BPD than similar groups with other PD, and substance use disorder is significantly less common in men with BPD—while rates are more similar among women.
19. An IQ above 130 is one of several traits that predict a better long-term outcome for people with BPD (source)
Borderline personality disorder statistics indicate certain traits strongly predict whether a person with BPD will fare better—or worse—than average. Poor outcomes include chronic functional impairment or completed suicide.
Traits linked to better-than-average outcomes:
- High intelligence (IQ over 130)
- Exceptional artistic talent
- Physical attractiveness as perceived by others (in women only)
- Obsessive-compulsive traits that promote strong self-discipline, productive work habits, and structured use of free time
- Sustained involvement in support groups like Alcoholics Anonymous (for those with substance use issues)
Traits linked to worse-than-average outcomes:
- History of severe trauma, such as transgenerational incest or parental brutality
- Untreated substance use disorders
- Schizotypal or antisocial personality traits
While BPD is challenging, certain protective traits and sustained treatment efforts can significantly improve long-term outcomes.
20. Half of people with BPD recover within 10 years—and even more people achieve symptom remission (source)
A 10-year prospective study found that 50% of BPD patients reached full recovery, defined as both symptom remission and good social and vocational functioning for at least two years. Additionally, 93% experienced symptomatic remission lasting two years, and 86% maintained remission for at least four years.
However, BPD can recur: 34% of those who recovered and 30% of those in remission relapsed after two years. It’s important to note that most participants received therapy or medication, so these findings may not reflect the course of untreated BPD. Still, the data challenges the outdated view of BPD as a lifelong, unchanging condition.
What These Borderline Personality Disorder Statistics Reveal
These BPD statistics present a nuanced picture of a complex condition—one that affects millions but also responds to early intervention, targeted therapies, and ongoing support. Here are some key takeaways from the data:
- BPD is more common than many realize, with estimates ranging from 1.6% to 5.9% of the U.S. population.
- Women are diagnosed more often, but this may reflect biases in how symptoms are interpreted, not actual prevalence.
- Suicide risk is alarmingly high, with up to 10% of people with BPD dying by suicide and 75% attempting it at least once.
- Childhood trauma is a major risk factor, especially abuse, neglect, and unstable family environments.
- Comorbidities are common and complicate treatment of BPD, particularly bipolar disorder, ADHD, and substance abuse.
- Adolescents are not immune, and early signs often emerge in teens with emotional or behavioral challenges.
- Not all traits predict the same outcomes—protective factors like high IQ, creativity, and structured habits can improve prognosis, while trauma and antisocial traits can worsen it.
- Treatment works—but not for everyone. Nearly 50% don’t fully respond to therapy, but newer approaches and personalized care continue to evolve.
- Recovery is possible: Half of people with BPD achieve full recovery within 10 years, and many more experience extended periods of remission.
While BPD remains a serious and often misunderstood condition, the data offers hope. With proper support, tailored treatment, and attention to both risk and resilience factors, many people with BPD go on to lead stable, fulfilling lives. BPD is not a life sentence—recovery is real and within reach.
How eCare Behavioral Health Institute Can Help
Understanding the complexities behind BPD and related personality disorder statistics is key to providing effective care—and continuing education can make all the difference. At eCare Behavioral Health Institute, you’ll find CEU-approved courses that deepen your knowledge of BPD diagnosis and treatment, from DBT techniques to other strategies for therapeutic success.
Learn at your own pace with expert-led, on-demand or live webinars, and easily track your progress with a user-friendly dashboard. Whether you’re a counselor, psychologist, clinician, or social worker, our wide range of online continuing education courses for mental health professionals is designed to help you stay current—not just with BPD, but with the full spectrum of mental health conditions encountered in practice.

